We are no longer offering surgery or consultations.
|
Techniques & Expectations
Surgical techniques
used for penile enlargement (enhancement phalloplasty) --
penile lengthening and penile widening (girth enhancement)
-- have been in the urologic literature for many years.
There are various
ways of enlarging the penis. In my practice, patients either
have a lengthening or widening alone, or a lengthening and
widening in a single session. Glanular enhancement may be
performed alone or combined with any procedure.
PENILE
LENGTHENING
Click to see before
and after photos of lengthening procedures:
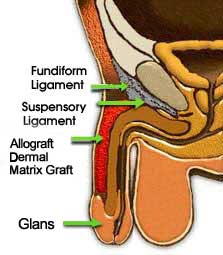
Approximately one-third
to one-half of the penis is inside the body, and is internally
attached to the undersurface of the pubic bone. Penile
lengthening involves the release of the fundiform ligament and the suspensory
ligament that attaches the 2 erectile bodies to the pubic
bone. The suspensory ligament makes the penis arch under the
pubic bone. Release of this ligament allows the penis to protrude
on a straighter path, further outward to give more functional
length. I use a 1" to 1½" lower abdominal incision
in the pubic hair area for concealment or a new incision
in the penile-pubic crease for concealment. This is a relatively
minor procedure. There will be no scar on the penis and there
is no possibility of pubic hair on the penis. I highly recommend
use of specially designed penile
weights
to maximize penile lengthening.
Penile length
gain in the flaccid state.
Average expected
length gain is 1 inch. Well motivated patients may gain up
to 2 inches. After Allograft
dermal matrix graft widening, the penis does not shrink
to its original small flaccid length, but stays slightly longer.
Penile length
gain in the erect state.
Usually there is
a slightly smaller penile length gain in the erect state than
in the flaccid state.
PENILE
WIDENING (PERICAVERNOSAL)
Click to see before and after photos of widening procedures:
We have noticed a permanent
increase in penile girth (circumference) in the flaccid
state with our pericavernosal (P/C) Allograft
dermal matrix graft technique. While a 40 to 50% gain
in girth (flaccid state) may be achieved, most men get an
increase of about 30%.
Because autograft
dermal fat grafts for penile widening require a donor site(s)
and, therefore, incision(s) and scar(s) --- 6 years ago I
stopped using autograft dermal fat grafts and since then only
use Allograft Dermal
Matrix Grafts (Alloderm®) in my patients who wish
penile widening.
The advantages of
Allograft Dermal
Matrix Grafts (Alloderm®) over autograft dermal fat
grafts are: it eliminates the need for incisions and scars
at the donor sites (because there are none) and it significantly
reduces the length of surgery.
With the Allograft
dermal matrix graft technique we are adding multiple layers
of Allograft dermal
matrix graft under the penile skin on top of the erectile
chambers to give thickness by "stacking" or "folding" the
grafts. I do not use strips of Allograft
dermal matrix graft, but create a conjoined graft.
There are no contour defects and appearance and feel are normal.
A penile stretching device is suggested after the widening
procedure to combat Allograft
dermal matrix graft contraction that might occur.
I have found this
technique to be effective with a high satisfaction rate.
These procedures
are performed in an outpatient ambulatory setting, either
at a hospital or in a private surgical facility. State licensed
personnel use a combination of anesthetic techniques that
will assure you a painless experience.
SECONDARY
AND TERTIARY PENILE WIDENING (PERICAVERNOSAL)
Click to see before and after photos of widening
procedures:
Sometimes
a patient who has had penile widening by:
liposuction/lipotransfer (fat injection) or
autograft dermal fat graft or Allograft
Dermal Matrix Graft (Alloderm ®) (pericavernosal)
wants additional girth enhancement.
During
the last six years I have used my Allograft
Dermal Matrix Graft (Alloderm ®) penile
widening technique to insert Allograft
Dermal Matrix Graft (Alloderm ®) above
or below the previously inserted graft(s)
with very satisfactory results in patients
who had one or a combination of the
above widening procedures.
GLANULAR ENHANCEMENT
Click to see before
and after photos of glanular enhancement procedures:
Glanular enhancement
is a relatively new surgical technique. Very few surgeons
around the world are performing it. However, it can be done
successfully with the Allograft
dermal matrix graft.
A reasonable expectation
is between 15% and 20% increase in the flare of the glans.
If performed with penile widening, no additonal incision is
required. A penile stretching device is not necessary
after this procedure.
FLACCID
PENILE STRAIGHTENING
Some men have penile
curvature in the flaccid state only. This can be corrected
without surgery on the erectile chambers by insertion of Allograft
Dermal Matrix Graft (Alloderm ®) when used for penile
widening.
Click to see before
and after photos of flaccid penile straightening:
PENILE
GLANULAR DISPROPORTION
Click
to see before and after photos of correction of penile glanular
disproportion:
PENOSCROTAL
WEBBING
If
the scrotum extends along the underside of the penis it
may make the penis appear short on the underside, like a
"turkey neck." This can be corrected by various techniques
under local anesthesia, or at the same time as penile lengthening
or penile widening or glanular enhancement.
Click
to see before and after photos of correction of penoscrotal
webbing:
SCROTAL
REDUCTION
If the scrotum
becomes enlarged due to age or is perceived to be too
large it may be reduced under local anesthesia.
FORESKIN
MODIFICATION
The foreskin
can be modified to a: (1) Standard Circumcision (2) High
Circumcision or (3) Low Circumcision.
REDUCTION
OF INFRAPUBIC AND SUPRAPUBIC FAT PAD
If the pubic area
has excess fat due to increased pubic or suprapubic fat the
penile shaft may be partially or completely hidden. Various
procedures can make the penis more visible. These procedures
are usually performed at the same time as penile lengthening
or penile widening.
LIPOSUCTION
AND FAT INJECTION TECHNIQUE
Since 1991, surgeons
have performed liposuction and fat injection into the penis.
While this can temporarily widen the penis, in the long run,
I find this procedure unpredictable. It often results in penile
irregularity and the augmentation always decreases with time.
During an erection the injected fat will be softer than engorged
tissue that hardens the penis.
Men who are particularly
poor candidates for this technique are those with litte body
fat (lean men). These men are often: bodybuilders, weight
lifters, models, actors, and dancers. Often these men require
several injections over time to have more fat injected into
the penis.
I do not perform
this procedure.
Click
on the patients below to view before and after photos of patients
that have experienced penis irregularity and penis deformity
after liposuction and fat injection into the penis. Patient
2, Patient 4, Patient
5, Patient 6, Patient
7 and Patient 8.
The frequency of
complications is not known because there are no large-scale
studies reported in the medical literature. Consequently,
some physicians consider these procedures to be experimental
or investigational.
The following complications
from penile lengthening and Allograft
dermal matrix graft widening (pericavernosal) are theoretically
possible:
- Loss of erect upward angle
of the penis. This has occurred in two of my patients.
- Keloid scars (a thick scar).
This is unusual but can often be treated by injections
of medication.
- Scarring causing a shorter
penis. I have never seen lasting shortness in my patients
who use a penile stretching device.
- Absorption of the Allograft
dermal matrix graft with loss of thickness. I have
seen one patient who had partial absorption and some loss
of thickness.
- Contracture
and/or separation of the Allograft
Dermal Matrix Graft (Alloderm ®).
I have seen one patient with partial
contracture of the graft, one patient
with proximal graft separation, and
one patient with distal separation
and contracture of the graft.
- Failure of the Allograft
dermal matrix graft to "take". This has not occurred
any of my patients.
- Skin incision separation.
I have seen slight temporary skin incision separation
in a few of my patients.
- Loss of some penile skin.
This rarely occurs.
- Bleeding. I have seen one
patient with a collection of blood under the skin that
was easily managed.
- Fibrosis of superficial
vein. This rarely occurs and usually resolves by itself.
- Infection. I have seen three patients who developed an infection and lost the graft and one patient who lost part of the graft, and three patients who did not lose the graft.
- Ecchymosis (bruising).
This occasionally occurs and resolves by itself.
- Nerve injury resulting
in decrease of penile sensation. This has not occurred
in any of my patients.
- Edema (temporary swelling
of the skin). I have occasionally seen this in my patients.
- Seroma (collection of serum
under skin). This has not occurred in any of my patients.
- Erectile dysfunction (difficulty
with erection). This has not occurred in any of my patients.
If some of these complications occur, further surgery may
be required.
Some penile length
may be obtained by significant weight loss (greater than 35
lbs.) if a large infrapubic fat pad is present or by a penile
stretching device. Complications may be associated with these
forms of treatment. Also review Frequently
Asked Questions about penile enlargement surgery ( phalloplasty
).
Penile
Lengthening |
Penile Widening
| Glanular Enhancement |
Liposuction & Fat Injections | Allograft
Dermal Matrix Graft |
About the Doctor | About
the Office |
Letters From Patients |
Q & A - Phalloplasty | Home
|
©Copyright 1998-.
| |
Disclaimer:
The content, illustrations and references to penis
enlargement, penis lengthening, penis widening, penis straightening (Peyronie's disease), penile girth enlargement and glanular
enhancement in
this website are for informational purposes only.
The content is not intended to be a substitute for
professional medical advice, diagnosis or treatment.
|
|

